







































 Inquiry
Inquiry Customer service
Customer service

| Basic knowledge of radiation therapy | ||
| adddate��2017/7/27 11:24:40 author����վ Hits��6343 | ||
|
Radiation therapy or radiotherapy, often abbreviated RT, RTx, or XRT, is therapy using ionizing radiation, generally as part of cancer treatment to control or kill malignant cells and normally delivered by a linear accelerator. Radiation therapy may be curative in a number of types of cancer if they are localized to one area of the body. It may also be used as part of adjuvant therapy, to prevent tumor recurrence after surgery to remove a primary malignant tumor (for example, early stages of breast cancer). Radiation therapy is synergistic with chemotherapy, and has been used before, during, and after chemotherapy in susceptible cancers. The subspecialty of oncology concerned with radiotherapy is called radiation oncology. Radiation therapy is commonly applied to the cancerous tumor because of its ability to control cell growth. Ionizing radiation works by damaging the DNA of cancerous tissue leading to cellular death. To spare normal tissues (such as skin or organs which radiation must pass through to treat the tumor), shaped radiation beams are aimed from several angles of exposure to intersect at the tumor, providing a much larger absorbed dose there than in the surrounding, healthy tissue. Besides the tumour itself, the radiation fields may also include the draining lymph nodes if they are clinically or radiologically involved with tumor, or if there is thought to be a risk of subclinical malignant spread. It is necessary to include a margin of normal tissue around the tumor to allow for uncertainties in daily set-up and internal tumor motion. These uncertainties can be caused by internal movement (for example, respiration and bladder filling) and movement of external skin marks relative to the tumor position. Radiation oncology is the medical specialty concerned with prescribing radiation, and is distinct from radiology, the use of radiation in medical imaging and diagnosis. Radiation may be prescribed by a radiation oncologist with intent to cure ("curative") or for adjuvant therapy. It may also be used as palliative treatment (where cure is not possible and the aim is for local disease control or symptomatic relief) or as therapeutic treatment (where the therapy has survival benefit and it can be curative). It is also common to combine radiation therapy with surgery, chemotherapy, hormone therapy, immunotherapy or some mixture of the four. Most common cancer types can be treated with radiation therapy in some way. The precise treatment intent (curative, adjuvant, neoadjuvant therapeutic, or palliative) will depend on the tumor type, location, and stage, as well as the general health of the patient. Total body irradiation (TBI) is a radiation therapy technique used to prepare the body to receive a bone marrow transplant. Brachytherapy, in which a radioactive source is placed inside or next to the area requiring treatment, is another form of radiation therapy that minimizes exposure to healthy tissue during procedures to treat cancers of the breast, prostate and other organs. Radiation therapy has several applications in non-malignant conditions, such as the treatment of trigeminal neuralgia, acoustic neuromas, severe thyroid eye disease, pterygium, pigmented villonodular synovitis, and prevention of keloid scar growth, vascular restenosis, and heterotopic ossification. The use of radiation therapy in non-malignant conditions is limited partly by worries about the risk of radiation-induced cancers.
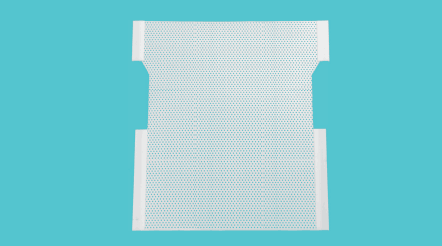
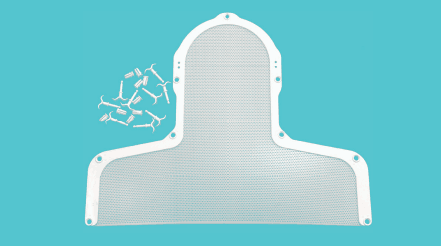
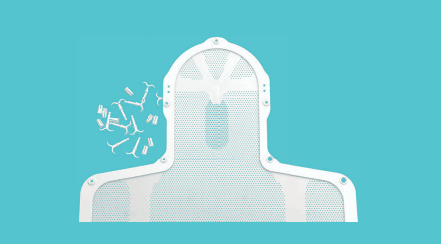
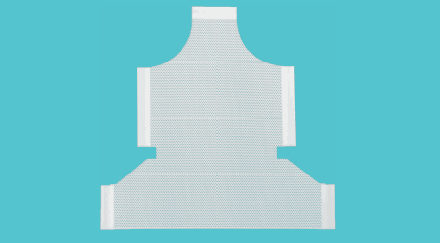
Medical usesDifferent cancers respond to radiation therapy in different ways. The response of a cancer to radiation is described by its radiosensitivity. Highly radiosensitive cancer cells are rapidly killed by modest doses of radiation. These include leukemias, most lymphomas and germ cell tumors. The majority of epithelial cancers are only moderately radiosensitive, and require a significantly higher dose of radiation (60-70 Gy) to achieve a radical cure. Some types of cancer are notably radioresistant, that is, much higher doses are required to produce a radical cure than may be safe in clinical practice. Renal cell cancer and melanoma are generally considered to be radioresistant but radiation therapy is still a palliative option for many patients with metastatic melanoma. Combining radiation therapy with immunotherapy is an active area of investigation and has shown some promise for melanoma and other cancers. It is important to distinguish the radiosensitivity of a particular tumor, which to some extent is a laboratory measure, from the radiation "curability" of a cancer in actual clinical practice. For example, leukemias are not generally curable with radiation therapy, because they are disseminated through the body. Lymphoma may be radically curable if it is localised to one area of the body. Similarly, many of the common, moderately radioresponsive tumors are routinely treated with curative doses of radiation therapy if they are at an early stage. For example: non-melanoma skin cancer, head and neck cancer, breast cancer, non-small cell lung cancer, cervical cancer, anal cancer, and prostate cancer. Metastatic cancers are generally incurable with radiation therapy because it is not possible to treat the whole body. Before treatment, a CT scan is often performed to identify the tumor and surrounding normal structures. The patient receives small skin marks to guide the placement of treatment fields. Patient positioning is crucial at this stage as the patient will have to be set-up in the identical position during treatment. Many patient positioning devices have been developed for this purpose, including masks and cushions which can be molded to the patient. The response of a tumor to radiation therapy is also related to its size. Due to complex radiobiology, very large tumors respond less well to radiation than smaller tumors or microscopic disease. Various strategies are used to overcome this effect. The most common technique is surgical resection prior to radiation therapy. This is most commonly seen in the treatment of breast cancer with wide local excision or mastectomy followed by adjuvant radiation therapy. Another method is to shrink the tumor with neoadjuvant chemotherapy prior to radical radiation therapy. A third technique is to enhance the radiosensitivity of the cancer by giving certain drugs during a course of radiation therapy. Examples of radiosensitizing drugs include: Cisplatin, Nimorazole, and Cetuximab. The effect of radiotherapy on control of cancer has been shown to be limited to the first five years after surgery, particularly for breast cancer. The difference between breast cancer recurrence in patients who receive radiotherapy vs. those who don't is seen mostly in the first 2�C3 years and no difference is seen after 5 years.
|
||
|
|
|
